KEY TAKEAWAYS for IUI Cycles
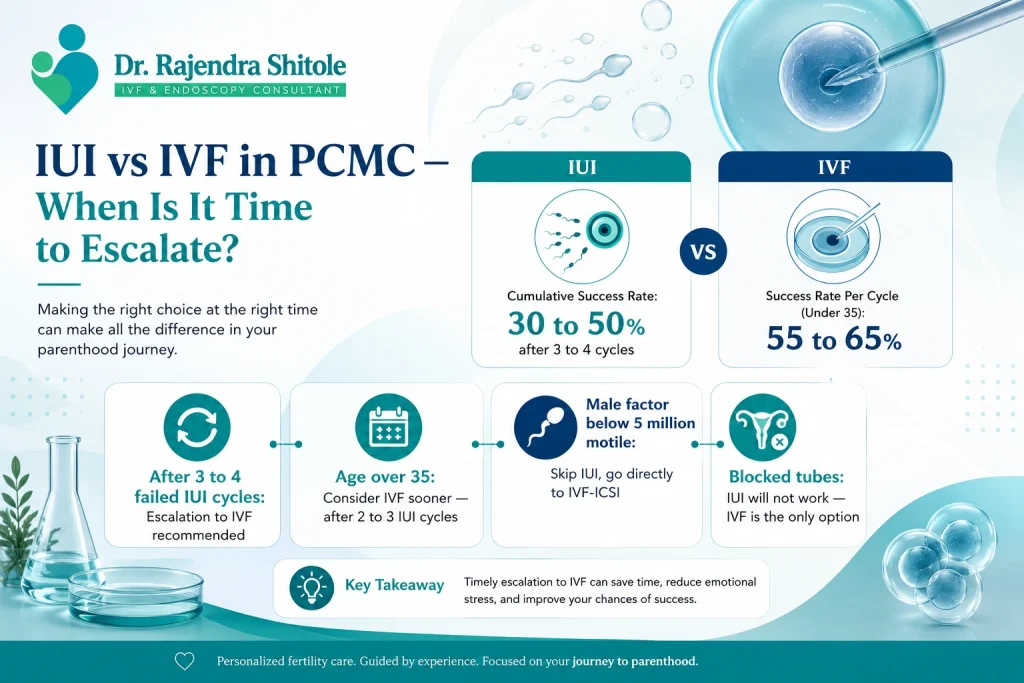
Most fertility specialists in PCMC recommend escalating from IUI to IVF after 3 to 4 failed IUI cycles.
IUI cumulative success rate plateaus after 4 cycles — continued IUI beyond this point rarely adds value.
Women over 35 should consider escalating to IVF earlier — after 2 to 3 failed IUI cycles.
Blocked fallopian tubes make IUI ineffective — IVF is the only appropriate treatment.
Severe male factor infertility (below 5 million total motile sperm) warrants direct IVF-ICSI without IUI attempts.
Dr. Shitole at his PCMC clinic reviews each IUI cycle outcome before recommending the next step.
When Should You Stop IUI and Move to IVF in PCMC?
How many IUI cycles before IVF in PCMC is one of the most common questions Dr. Shitole’s team receives. It’s a question loaded with hope, frustration and financial concern. The honest, evidence-based answer is: 3 to 4 cycles for most couples, sooner for those over 35 or with specific diagnoses that make IUI less likely to succeed.
IUI is an excellent first-line fertility treatment for the right candidates. But it has real limits. Understanding those limits — and knowing when to escalate — saves couples months or years of emotionally and financially costly treatment that is unlikely to succeed. This guide, reviewed by Dr. Rajendra Shitole — IVF and IUI specialist in PCMC — gives you the clinical evidence to make that decision confidently.
QUICK FACTS Of IUI Success Rate
- IUI Success Rate per Cycle (stimulated): 12 to 20 percent
- IUI Cumulative Success Rate (3 cycles): 30 to 50 percent
- IUI Cumulative Success Rate (beyond 4 cycles): Minimal additional benefit
- IVF Success Rate per Cycle (under 35): 55 to 65 percent
- Recommended IUI Attempts (standard cases): 3 to 4 cycles
- Recommended IUI Attempts (over 35): 2 to 3 cycles
PCMC IUI and IVF Escalation Statistics 2025-2026
| Metric | Data Point | Source |
| IUI success rate per cycle (stimulated) | 12 to 20 percent | ICMR 2024 |
| IUI cumulative success (3 cycles) | 30 to 50 percent | Industry estimate |
| IUI cumulative success (4 to 6 cycles) | Marginal improvement only | Industry estimate |
| IVF success rate per cycle (under 35) | 55 to 65 percent | ICMR 2024 |
| Recommended IUI escalation point | After 3 to 4 cycles | ICMR 2024 |
| IUI success rate over age 38 | Below 8 percent per cycle | Industry estimate |
| Couples who escalate after 3 cycles vs 6 | No significant outcome difference | PubMed 2020 |
The IUI Success Plateau — Why More Cycles Don’t Always Help
IUI has a success rate of 12 to 20 percent per stimulated cycle. After 3 to 4 cycles, the cumulative success rate reaches 30 to 50 percent. After that point, the curve flattens significantly. A couple who has had 5 IUI failures has roughly the same statistical profile on their 6th attempt as they did on their 5th — it’s not a cumulative upward journey.
The reason is that IUI works by improving the chance of a random event — sperm meeting egg. It doesn’t overcome the fundamental biological barriers that may be preventing pregnancy. IVF bypasses those barriers by creating the embryo in a controlled laboratory environment. For couples whose IUI cycles have failed despite apparently good conditions, IVF adds diagnostic value as well — it shows how eggs fertilise, how embryos develop and whether there are hidden factors at play.
When Should You Escalate to IVF Sooner in PCMC?
Several clinical situations make early IVF escalation the right choice — even before completing 3 to 4 IUI cycles:
| Clinical Situation | IUI Cycles Recommended | Reason for Early IVF |
| Age over 38 | 0 to 1 cycle | Success rate under 8 percent per IUI; every month matters |
| Age 35 to 37 | 2 to 3 cycles maximum | IVF significantly more effective; less time to waste |
| Blocked fallopian tube(s) | 0 — go directly to IVF | IUI requires open tubes to work |
| Severe male factor (below 5M TMC) | 0 — go directly to IVF-ICSI | IUI ineffective at this sperm count |
| Previous ectopic pregnancy | Caution — discuss with Dr. Shitole | IUI may increase ectopic risk in damaged tube |
| Diminished ovarian reserve (low AMH) | 0 to 2 cycles | Limited time window; IVF more efficient |
| 3 or more failed IUI cycles | Stop IUI, move to IVF | Success plateau reached |
What Happens During a Failed IUI Cycle Review?
At Dr. Shitole’s PCMC clinic, every failed IUI cycle is reviewed before the next step is recommended. The review covers:
- Follicle count and size at trigger — was stimulation optimal?
- Timing of insemination relative to ovulation — was the window accurate?
- Sperm parameters at wash — was total motile count adequate for IUI?
- Endometrial thickness at insemination — was the lining receptive?
- Post-procedure luteal phase support — was progesterone adequate?
This systematic review often reveals subtle factors that can be corrected in a subsequent cycle — or confirms that IUI has reached its limit for this couple and IVF is the right next step.
The Cost Calculation — IUI vs IVF in PCMC
| Scenario | Cost (INR) | Success Rate |
| 1 IUI cycle (stimulated) | 8,000 to 25,000 | 12 to 20 percent |
| 3 IUI cycles total | 24,000 to 75,000 | 30 to 50 percent cumulative |
| 4 IUI cycles total | 32,000 to 1,00,000 | Marginal gain over 3 |
| 1 IVF cycle (all inclusive) | 1,30,000 to 2,00,000 | 55 to 65 percent (under 35) |
| IVF after 3 failed IUI cycles | 1,54,000 to 2,75,000 total spend | Better efficiency overall |
For most couples, 3 IUI cycles followed by IVF if needed represents the most cost-efficient and time-efficient pathway. Extending to 6 IUI cycles before IVF costs more, takes longer and does not meaningfully improve total success rate (PubMed 2020).
A Real Decision From PCMC
A 34-year-old woman from Nigdi and her husband (mild oligospermia — 10 million total motile count) completed 3 stimulated IUI cycles at Dr. Shitole’s PCMC clinic over 9 months. Each cycle was well-managed — good follicles, good timing, adequate endometrial lining. All 3 failed. After a comprehensive review, Dr. Shitole recommended IVF-ICSI. On the first IVF cycle, 8 eggs were retrieved, 6 fertilised via ICSI and 2 blastocysts were transferred. The couple achieved a twin pregnancy. They were grateful they hadn’t tried a 4th or 5th IUI cycle.
IUI to IVF Escalation in PCMC — Local Context
PCMC couples often extend IUI attempts beyond what’s clinically advisable due to cost concerns — IVF’s higher upfront cost feels daunting compared to the lower per-cycle IUI fee. Dr. Shitole’s clinic offers transparent IVF cost consultations and, where clinically appropriate, financing options to make the transition from IUI to IVF as smooth as possible.
The PCMC IT workforce demographic — couples aged 28 to 36, time-pressured, career-focused — particularly benefits from efficient treatment pathways. Spending 12 months on 4 to 6 IUI cycles when IVF would have succeeded in month 4 is a real cost, both financially and emotionally.
Frequently Asked Questions
Q: How many IUI cycles should I try before switching to IVF in PCMC?
For most couples under 35, 3 to 4 stimulated IUI cycles is the evidence-based recommendation before escalating to IVF. For women over 35, 2 to 3 cycles. For those with blocked tubes, severe male factor or very low AMH, IVF should be considered immediately without IUI attempts.
Q: Why did my IUI fail even though everything looked good?
IUI has a 12 to 20 percent per-cycle success rate even under ideal conditions. A ‘good-looking’ cycle does not guarantee success because fertilisation and implantation involve biological processes that IUI cannot control. Repeated failure despite good IUI parameters is often the clearest signal that IVF is needed.
Q: Is it wasting money to do more than 3 IUI cycles before IVF?
Clinically speaking, yes for most couples. The additional probability of success from a 4th, 5th or 6th IUI cycle is small — and the cost of those cycles adds to your total IVF spend without meaningfully improving overall outcome. Dr. Shitole’s clinic will always discuss the cost-benefit analysis openly at each cycle review.
Q: Can IUI work after 3 failures if the doctor changes the protocol?
In some cases, yes. If a protocol change addresses a specific correctable factor — different stimulation dose, better-timed insemination, improved luteal support — a 4th IUI can be worth trying. Dr. Shitole reviews each failed cycle carefully before recommending continuation or escalation.
Q: Should I go directly to IVF if I’m 37 and have unexplained infertility?
Many fertility specialists, including Dr. Shitole, would recommend a maximum of 2 to 3 IUI cycles for a 37-year-old with unexplained infertility, followed by IVF if unsuccessful. At 37, every cycle matters and IVF’s significantly higher success rate per cycle justifies the higher cost.
Q: What does switching from IUI to IVF involve at Dr. Shitole’s PCMC clinic?
The transition is straightforward. If your IUI cycles have been at Dr. Shitole’s clinic, your existing test results and cycle records carry over. A fresh consultation reviews your current status, updates any outstanding tests (AMH, semen analysis) and maps out your IVF protocol. Most couples can start their IVF cycle within 4 to 6 weeks of making the decision.
Conclusion
How many IUI cycles before IVF in PCMC comes down to a clear evidence-based answer: 3 to 4 cycles for most couples, sooner if you’re over 35 or have specific diagnoses that limit IUI’s effectiveness. The IUI-to-IVF transition is not a failure — it’s a data-informed clinical upgrade.
Dr. Rajendra Shitole at D.Y. Patil Hospital, Pimpri-Chinchwad guides every PCMC couple through this decision with transparency, clinical rigour and deep respect for your time and emotional investment.
If you’ve had failed IUI cycles and are wondering what comes next, book a consultation today at drrajendrashitoleivfdoctor.com — and get a clear, personalised answer.

Dr. Rajendra Shitole
Dr. Rajendra Shitole, Best IVF & Fertility Specialist Centre in Kharadi, Pune .He is highly skilled Gynaecologist, Fertility Consultant, and Laparoscopic & Robotic Surgeon with over 11 years of experience dedicated to women’s health and reproductive care. His mission is to help childless couples fulfill their dream of parenthood through compassionate care and advanced medical expertise.
He has successfully managed numerous complex cases of Infertility, Fibroids, PCOS, Adenomyosis, Endometriosis, and Male Factor Infertility.