KEY TAKEAWAYS
Recurrent miscarriage is defined as two or more consecutive pregnancy losses — affecting approximately 1 to 2 percent of couples trying to conceive.
Chromosomal abnormalities in the embryo cause approximately 50 percent of all miscarriages — PGT-A testing identifies and excludes these before transfer.
Antiphospholipid syndrome (APS) — a blood clotting disorder — is a treatable cause of recurrent miscarriage found in 10 to 15 percent of cases.
Uterine structural abnormalities (polyps, fibroids, septum) are found in 15 to 20 percent of recurrent miscarriage patients on hysteroscopy.
IVF with PGT-A significantly reduces miscarriage rates by ensuring only chromosomally normal embryos are transferred.
Dr. Shitole’s PCMC clinic provides a comprehensive recurrent miscarriage investigation and treatment pathway.
What Is Recurrent Miscarriage and How Common Is It in PCMC?
Recurrent miscarriage and IVF in PCMC represents one of the most emotionally challenging fertility journeys Dr. Shitole’s team accompanies couples through. Recurrent pregnancy loss (RPL) is defined as two or more consecutive miscarriages before 20 weeks of gestation. It affects approximately 1 to 2 percent of couples trying to conceive (ICMR 2024). While a single miscarriage is common — affecting up to 15 to 20 percent of known pregnancies — recurrent loss signals an underlying cause that warrants investigation.
Most couples who experience recurrent miscarriage have a treatable or manageable underlying factor. Finding it requires a systematic investigation. Dr. Rajendra Shitole at D.Y. Patil Hospital, PCMC guides couples through this process with clinical rigour and deep compassion — because recurrent miscarriage is not just a medical diagnosis. It’s a grief that accumulates.
QUICK FACTS OF RECURRENT MISCARRIAGE
- Recurrent Miscarriage Prevalence: 1 to 2 percent of couples (ICMR 2024)
- Chromosomal Cause Share: Approx. 50 percent of miscarriages
- APS (Blood Clotting Disorder) in RPL: 10 to 15 percent of cases
- Uterine Abnormality in RPL: 15 to 20 percent on hysteroscopy
- PGT-A Miscarriage Rate Reduction: Up to 50 percent in chromosomal RPL
- Live Birth Rate After IVF With PGT-A in RPL: 60 to 70 percent
PCMC Recurrent Miscarriage Statistics 2025-2026
| Metric | Data Point | Source |
| Recurrent miscarriage prevalence | 1 to 2 percent of couples | ICMR 2024 |
| Chromosomal cause of miscarriage | Approx. 50 percent | PubMed 2021 |
| APS as RPL cause | 10 to 15 percent of cases | ICMR 2024 |
| Uterine abnormality in RPL | 15 to 20 percent | Industry estimate |
| Unexplained RPL proportion | 25 to 30 percent | Industry estimate |
| PGT-A miscarriage rate reduction | Up to 50 percent | PubMed 2022 |
| Live birth rate after IVF with PGT-A in RPL | 60 to 70 percent | Industry estimate |
Causes of Recurrent Miscarriage — What the Investigation Looks For
| Cause Category | Specific Condition | Proportion | Treatment |
| Chromosomal | Embryo aneuploidy (random) | 50 percent of losses | PGT-A to select normal embryos |
| Chromosomal | Parental structural chromosome abnormality | 3 to 5 percent of couples | Genetic counselling, IVF with PGT |
| Anatomical | Uterine septum, polyps, fibroids, adhesions | 15 to 20 percent | Hysteroscopic correction |
| Thrombophilic | APS, Factor V Leiden, thrombophilia | 10 to 15 percent | Heparin and aspirin in pregnancy |
| Hormonal | Thyroid disorders, high prolactin, diabetes | 5 to 10 percent | Hormonal correction before conception |
| Immunological | Elevated NK cells, alloimmune factors | 5 to 10 percent | Immunotherapy protocols in IVF |
| Unexplained | No identifiable cause found | 25 to 30 percent | Empirical treatment, PGT-A, lifestyle |
The Recurrent Miscarriage Investigation at Dr. Shitole’s PCMC Clinic
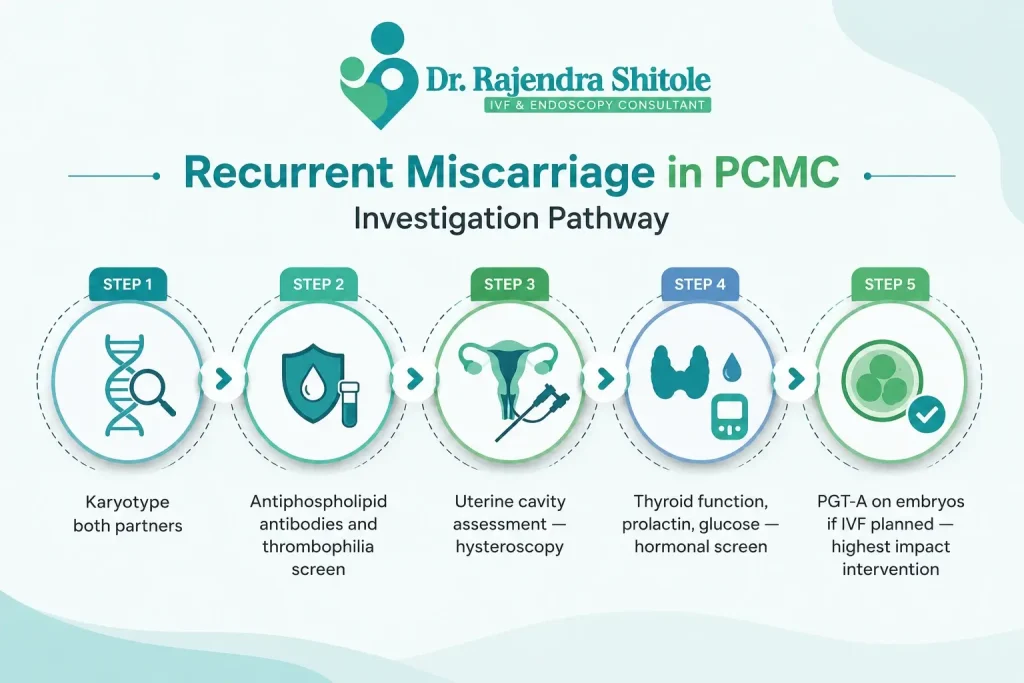
A structured investigation is the foundation of effective RPL management. At Dr. Shitole’s PCMC clinic, the standard RPL workup includes:
- Karyotype of both partners — identifies structural chromosomal abnormalities in either parent
- Antiphospholipid antibody panel (ACA and lupus anticoagulant) on two occasions, 12 weeks apart — diagnoses APS
- Thrombophilia screen — Factor V Leiden, prothrombin gene mutation, protein C and S, antithrombin III
- Thyroid function tests (TSH, Free T4) and prolactin — hormonal causes
- Fasting glucose and HbA1c — excludes diabetes
- Uterine cavity assessment — hysteroscopy or saline infusion sonography
- Sperm DNA fragmentation — elevated DFI is associated with early pregnancy loss
How IVF With PGT-A Helps Recurrent Miscarriage Patients in PCMC
The single most effective intervention for recurrent miscarriage caused by chromosomal factors is IVF with PGT-A (Preimplantation Genetic Testing for Aneuploidies). PGT-A involves biopsying a few cells from each blastocyst and analysing the chromosomes of all 24 chromosomes. Only chromosomally normal (euploid) embryos are transferred.
For couples with recurrent miscarriage — where chromosomal embryo abnormality is the most common underlying cause — PGT-A reduces the miscarriage rate by up to 50 percent (PubMed 2022) and delivers live birth rates of 60 to 70 percent per transfer in selected patients. The cost of PGT-A in PCMC is INR 30,000 to 50,000 in addition to the IVF cycle cost.
Antiphospholipid Syndrome and Recurrent Miscarriage — A Treatable Cause
Antiphospholipid syndrome (APS) is an autoimmune condition where antibodies attack phospholipids in blood vessel walls, causing clotting that obstructs the placental blood supply. This deprives the early embryo of nutrients and oxygen, causing pregnancy loss — often at 10 to 14 weeks when the placenta becomes the primary blood supply.
APS is diagnosed by finding antiphospholipid antibodies on two tests, 12 weeks apart. Treatment is straightforward and highly effective: low-molecular-weight heparin injections and low-dose aspirin started at the time of embryo transfer or positive pregnancy test, continued through 36 weeks. With treatment, the majority of APS patients achieve successful pregnancies.
Emotional Support for Recurrent Miscarriage Patients at Dr. Shitole’s PCMC Clinic
Recurrent miscarriage is cumulative grief. Each loss is not just a clinical event — it’s the end of a pregnancy that was already a baby in the minds of the parents. Dr. Shitole’s clinic provides dedicated psychological counselling support for recurrent miscarriage patients, separate from clinical consultations. This is not optional — it’s part of the care pathway.
Indian families often add social pressure to biological grief. Family members asking ‘when will you have a child’ after multiple losses is a real and painful experience for many PCMC couples. Dr. Shitole’s counselling team helps couples communicate boundaries, manage expectations and protect their emotional health through the investigation and treatment process.
Recurrent Miscarriage and IVF in PCMC — Local Context
Women in PCMC who experience recurrent miscarriage often wait longer than necessary before seeking specialist care — partly due to cultural normalisation of early pregnancy loss and partly due to lack of awareness that investigation after two losses is now the recommended standard (ICMR 2024). Dr. Shitole’s clinic actively promotes early investigation through community outreach and social media in the PCMC area.
Couples from Wakad, Hinjewadi, Nigdi, Bhosari, Chinchwad and Akurdi access recurrent miscarriage investigation and IVF services at D.Y. Patil Hospital. The investigation panel can usually be completed within one menstrual cycle, and treatment — if warranted — can begin within 4 to 6 weeks of the workup.
Frequently Asked Questions
Q: What is considered recurrent miscarriage in PCMC?
Two or more consecutive pregnancy losses before 20 weeks is the current definition of recurrent miscarriage (ICMR 2024). Some specialists begin investigation after two losses; others wait for three. Dr. Shitole recommends beginning the workup after two consecutive losses — because treatable causes can be found and corrected before a third loss occurs.
Q: Does IVF prevent miscarriage?
IVF with PGT-A significantly reduces miscarriage rates in couples with chromosomal RPL — by up to 50 percent (PubMed 2022). For couples with APS, heparin and aspirin treatment during pregnancy reduces miscarriage rates dramatically. IVF itself does not prevent miscarriage — but the tools available within IVF (PGT-A, personalised protocols) address the most common causes.
Q: Can I get pregnant again after recurrent miscarriage?
Yes. The majority of couples with recurrent miscarriage go on to have a successful pregnancy once the underlying cause is identified and treated. Even in unexplained RPL, live birth rates with supportive care and optimised IVF protocols are 60 to 70 percent (Industry estimate). Early investigation and treatment is the key.
Q: How much does PGT-A cost in PCMC?
PGT-A in PCMC costs INR 30,000 to 50,000 in addition to the IVF cycle cost. This covers biopsy of blastocysts, chromosomal analysis of all 24 chromosomes and results reporting. The cost is per batch of embryos tested, not per individual embryo.
Q: Is there treatment for unexplained recurrent miscarriage?
A: For unexplained RPL, Dr. Shitole uses an empirical approach: PGT-A to screen embryos, ERA-guided transfer timing, low-dose aspirin and progesterone support, and immunological protocols where NK cell activity is elevated. Lifestyle optimisation — BMI correction, thyroid normalisation, stress reduction — also plays a role. Even without a clear cause, most couples achieve a successful pregnancy with this comprehensive approach.
Q: Should I have a hysteroscopy after recurrent miscarriage?
A: Yes. Hysteroscopy is a standard part of the recurrent miscarriage workup at Dr. Shitole’s PCMC clinic. Uterine abnormalities — polyps, a uterine septum, adhesions — are found in 15 to 20 percent of RPL patients (Industry estimate) and are entirely correctable. A 30-minute hysteroscopy can identify and treat these in one sitting.
Conclusion
Recurrent miscarriage and IVF in PCMC are deeply connected. IVF with PGT-A, combined with systematic investigation and targeted treatment of underlying causes, offers the most effective path forward for couples who have experienced multiple pregnancy losses.
Dr. Rajendra Shitole at D.Y. Patil Hospital, Pimpri-Chinchwad provides a comprehensive recurrent miscarriage investigation and treatment programme — bringing together clinical expertise, genetic testing, immunological protocols and dedicated counselling support.
If you’ve experienced two or more miscarriages, please don’t wait for another loss before seeking investigation.
Book your RPL consultation at drrajendrashitoleivfdoctor.com today.
You deserve answers. You deserve support. And you deserve to know that for most couples in your situation, the path to a successful pregnancy exists — it just needs to be found.

Dr. Rajendra Shitole
Dr. Rajendra Shitole, Best IVF & Fertility Specialist Centre in Kharadi, Pune .He is highly skilled Gynaecologist, Fertility Consultant, and Laparoscopic & Robotic Surgeon with over 11 years of experience dedicated to women’s health and reproductive care. His mission is to help childless couples fulfill their dream of parenthood through compassionate care and advanced medical expertise.
He has successfully managed numerous complex cases of Infertility, Fibroids, PCOS, Adenomyosis, Endometriosis, and Male Factor Infertility.