KEY TAKEAWAYS
Azoospermia — zero sperm in ejaculate — affects 10 to 15 percent of infertile men and is not always a permanent barrier to fatherhood.
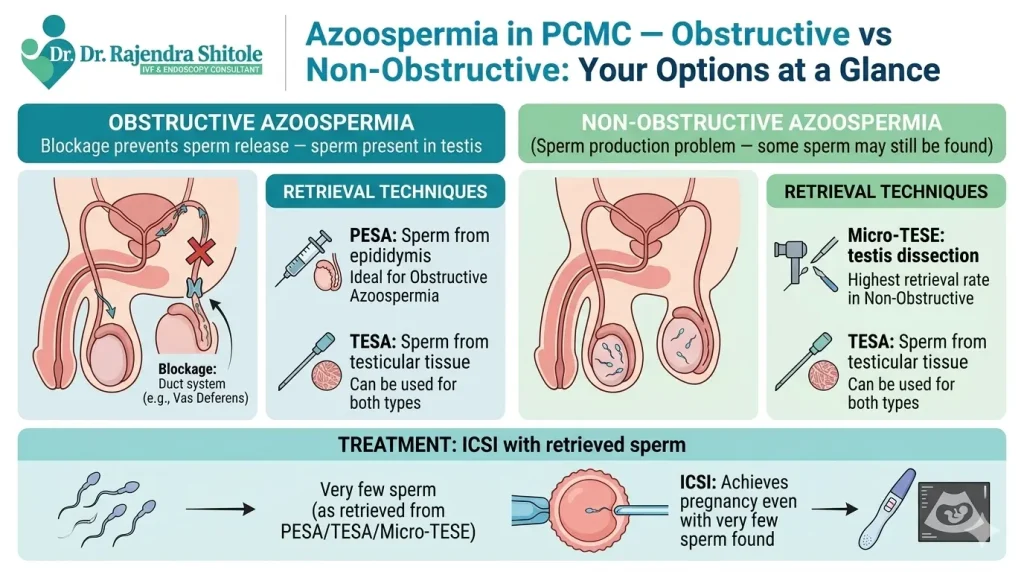
Obstructive azoospermia (40 percent of cases) almost always has sperm retrievable via PESA or TESA.
Non-obstructive azoospermia (60 percent) has a 50 to 60 percent chance of finding sperm via micro-TESE.
Retrieved sperm are used for ICSI — even a single viable sperm can fertilise an egg.
TESA procedure cost in PCMC is INR 15,000 to 30,000; combined IVF-ICSI with TESA costs INR 1,50,000 to 2,20,000.
Dr. Shitole performs TESA and PESA at his PCMC clinic at D.Y. Patil Hospital, Pimpri-Chinchwad.
What Is Azoospermia and How Common Is It in PCMC?
Azoospermia treatment in PCMC is available — and the outcomes for many men are better than they expect. Azoospermia is defined as the complete absence of sperm in the ejaculate on two separate semen analyses. It affects approximately 10 to 15 percent of infertile men (Industry estimate) and is one of the most challenging yet ultimately treatable male fertility conditions.
The key distinction is between obstructive and non-obstructive azoospermia. In obstructive cases, sperm are produced normally in the testis but cannot reach the ejaculate due to a blockage. In non-obstructive cases, sperm production itself is impaired. Both types have treatment options — with different procedures and success rates. This guide, reviewed by Dr. Rajendra Shitole, explains everything PCMC men and their partners need to know.
QUICK FACTS
Azoospermia Prevalence in Infertile Men: 10 to 15 percent (Industry estimate)
Obstructive Azoospermia Share: Approx. 40 percent of azoospermia cases
Non-Obstructive Azoospermia Share: Approx. 60 percent
TESA Sperm Retrieval Success (Obstructive): Near 100 percent
Micro-TESE Success (Non-Obstructive): 50 to 60 percent
TESA Procedure Cost PCMC: INR 15,000 to 30,000
PCMC Azopermia Statistics 2025-2026
| Metric | Data Point | Source |
| Azoospermia prevalence in infertile men | 10 to 15 percent | Industry estimate |
| Obstructive azoospermia share | Approx. 40 percent | ICMR 2024 |
| Non-obstructive azoospermia share | Approx. 60 percent | ICMR 2024 |
| TESA success rate (obstructive) | Near 100 percent | Industry estimate |
| Micro-TESE success rate (non-obstructive) | 50 to 60 percent | Industry estimate |
| IVF-ICSI success with TESA sperm | 35 to 50 percent per cycle | Industry estimate |
| TESA procedure cost PCMC | INR 15,000 to 30,000 | Industry estimate |
Obstructive vs Non-Obstructive Azoospermia — Key Differences
| Feature | Obstructive Azoospermia | Non-Obstructive Azoospermia |
| Sperm production | Normal — sperm are made | Impaired — reduced or absent production |
| Cause | Blockage in vas deferens or epididymis | Hormonal, genetic or testicular failure |
| Testicular size | Usually normal | Often smaller |
| FSH levels | Usually normal | Often elevated |
| Sperm retrieval success | Near 100 percent with PESA/TESA | 50 to 60 percent with micro-TESE |
| Common causes | Vasectomy, infection, congenital absence of vas | Klinefelter syndrome, cryptorchidism, chemotherapy |
| Best procedure | PESA or TESA | Micro-TESE |
Sperm Retrieval Options for Azoospermia at Dr. Shitole’s PCMC Clinic
PESA — Percutaneous Epididymal Sperm Aspiration
PESA is a simple, minimally invasive procedure performed under local anaesthesia or IV sedation. A fine needle is inserted into the epididymis (the tube behind the testis that stores sperm) and sperm are aspirated directly. It takes 15 to 20 minutes and is the first-choice procedure for obstructive azoospermia. PESA cost in PCMC: INR 10,000 to 20,000.
TESA — Testicular Sperm Extraction
TESA uses a fine needle to aspirate tissue directly from the testicular parenchyma. It is used in both obstructive and some non-obstructive cases. Multiple passes from different areas of the testis are made to maximise sperm retrieval. Sperm found are used immediately for ICSI or can be frozen for future use. TESA cost in PCMC: INR 15,000 to 30,000.
Micro-TESE — Microsurgical Testicular Sperm Extraction
Micro-TESE is the most advanced sperm retrieval technique. An operating microscope is used to identify and excise small areas of testicular tissue that appear to have active sperm production — identifiable as slightly opaque, plumper tubules. This maximises the chance of finding sperm in non-obstructive azoospermia while minimising damage to testicular tissue.
Micro-TESE offers a 50 to 60 percent sperm retrieval rate in non-obstructive azoospermia (Industry estimate) — far higher than conventional TESA. Procedure cost in PCMC: INR 30,000 to 60,000.
What Happens After Sperm Is Retrieved — IVF-ICSI in PCMC
Retrieved sperm — whether fresh or frozen — are used for ICSI. A single viable sperm is injected directly into each mature egg. Even sperm with poor motility or abnormal appearance can often be used for ICSI as long as they are alive. The fertilised embryos are then cultured to blastocyst stage and transferred to the female partner’s uterus.
IVF-ICSI success with surgically retrieved sperm in PCMC is 35 to 50 percent per cycle (Industry estimate). This is slightly lower than cycles with ejaculated sperm because retrieved sperm, particularly from non-obstructive cases, may have lower DNA integrity. Dr. Shitole’s embryology team accounts for this with careful sperm selection under high magnification.
Pre-Operative Assessment for Azoospermia Surgery in PCMC
- Hormonal profile: FSH, LH, testosterone, prolactin — differentiates obstructive from non-obstructive
- Genetic testing: Karyotype, Y-chromosome microdeletion analysis — essential for non-obstructive azoospermia
- Scrotal ultrasound: Testicular volume, epididymis assessment, varicocele check
- Anaesthesia assessment: For TESA and micro-TESE under IV sedation or GA
- Female partner workup: AMH, AFC, uterine assessment — to time sperm retrieval with IVF cycle
Azoospermia Treatment in PCMC — Local Context
Men in PCMC with azoospermia often delay seeking treatment due to stigma around male infertility. Dr. Shitole’s clinic at D.Y. Patil Hospital, Pimpri-Chinchwad offers confidential, non-judgmental male fertility consultations. The entire process — from semen analysis to TESA and IVF-ICSI — is managed at one centre, reducing the logistical burden for couples from Wakad, Hinjewadi, Nigdi, Chinchwad, Bhosari and Akurdi.
A man from Bhosari, PCMC, came to Dr. Shitole’s clinic after his semen analysis returned a result of zero sperm. His FSH was mildly elevated and testicular volume was borderline reduced. Genetic testing showed no Klinefelter syndrome or Y-deletion. A TESA procedure found motile sperm in two of six needle passes. These were frozen and used in his wife’s IVF-ICSI cycle. The couple achieved a successful pregnancy on their first attempt.
Frequently Asked Questions
Q: Can a man with zero sperm count father a biological child in PCMC?
A: In many cases, yes. Obstructive azoospermia almost always has retrievable sperm via PESA or TESA. Non-obstructive azoospermia has a 50 to 60 percent chance of sperm being found via micro-TESE. Retrieved sperm are used for ICSI — even a single viable sperm is sufficient to fertilise an egg.
Q: What is the difference between TESA and micro-TESE?
A: TESA uses a fine needle to aspirate testicular tissue blindly from multiple sites. Micro-TESE uses an operating microscope to identify and selectively excise areas of the testis most likely to contain sperm — particularly dilated, opaque tubules. Micro-TESE has a higher success rate in non-obstructive azoospermia and causes less testicular damage.
Q: What causes azoospermia?
A: Obstructive azoospermia is caused by blockages — vasectomy, infections (chlamydia, gonorrhoea), congenital absence of the vas deferens (associated with CFTR gene mutations). Non-obstructive causes include Klinefelter syndrome, Y-chromosome microdeletions, chemotherapy, radiation, cryptorchidism (undescended testis) and idiopathic testicular failure.
Q: Is TESA painful?
A: TESA at Dr. Shitole’s PCMC clinic is performed under IV sedation — you are comfortable throughout. Post-procedure scrotal discomfort is mild and managed with ice packs and oral analgesics for 24 to 48 hours. Most men return to desk work within 2 to 3 days.
Q: What is the cost of azoospermia treatment and IVF in PCMC?
A: PESA costs INR 10,000 to 20,000 and TESA costs INR 15,000 to 30,000. Micro-TESE costs INR 30,000 to 60,000. Combined IVF-ICSI with surgically retrieved sperm costs INR 1,50,000 to 2,20,000 all inclusive. An itemised estimate is provided at consultation.
Q: Should I freeze sperm retrieved during TESA?
A: Yes, where possible. Freezing excess retrieved sperm allows future FET cycles without repeating the surgical procedure. Dr. Shitole’s embryology team cryopreserves all viable retrieved sperm not used in the immediate cycle. Annual storage costs apply.
Conclusion
Azoospermia treatment in PCMC in 2026 offers genuine hope for men who were once told biological fatherhood was impossible. With PESA, TESA and micro-TESE at Dr. Shitole’s D.Y. Patil Hospital clinic, combined with IVF-ICSI, a significant proportion of azoospermic men in PCMC have gone on to father biological children.
The first step is a thorough assessment — hormonal profile, genetic testing and scrotal ultrasound — to determine which type of azoospermia you have and which procedure gives you the best chance.
Book Your Male Fertility Consultation With Dr Rajendra Shitole

Dr. Rajendra Shitole
Dr. Rajendra Shitole, Best IVF & Fertility Specialist Centre in Kharadi, Pune .He is highly skilled Gynaecologist, Fertility Consultant, and Laparoscopic & Robotic Surgeon with over 11 years of experience dedicated to women’s health and reproductive care. His mission is to help childless couples fulfill their dream of parenthood through compassionate care and advanced medical expertise.
He has successfully managed numerous complex cases of Infertility, Fibroids, PCOS, Adenomyosis, Endometriosis, and Male Factor Infertility.